|
This article was written by Rene S. Cabral-Daniels, CEO of Community Care Network of Virginia, Inc., for the December 2016 edition of “Networking News.” The Network Technical Assistance Project is funded by the Federal Office of Rural Health Policy, Health Resources and Services Administration, U.S. Department of Health and Human Services through a contract to Rural Health Innovations, LLC, a subsidiary of the National Rural Health Resource Center Recent healthcare literature is replete with articles regarding the importance of paying greater attention to healthcare data. Many suggest a healthcare organization’s ability to harness data value is the fulcrum to the organization’s success or failure. While these articles encourage greater use of healthcare data, they often fail to inform health entities of the importance of assuring proper data ownership as well as stewardship, integrity and dissemination. Data requirements: what they are and what they aren’t Healthcare leaders may mistakenly believe that compliance with the Health Insurance Portability and Accountability Act (HIPAA) health data protection sections insulate them from any potential legal claims. HIPAA is an important, albeit complex, federal law that addresses both health data protection as well as confidential handling of protected health information (PHI). The determination of data ownership as well as necessary PHI protection is further complicated by the use of electronic health records (EHR). Health records no longer reside on a shelf in a doctor’s office but can now be shared by few keystrokes on a computer. EHR usage changes the parameters of astute data governance responsibility from one concerned with data ownership to one focused on data stewardship. Recent legislation promoting quality-based payments such as the Medicare Access & CHIP Reauthorization Act (MACRA) and the 824-page final rule describing implementation assure the use of electronic health records will continue to grow. The parameters of this growth are carefully prescribed in section 1848(o)(2)(A)(iii) of MACRA and the definition of “meaningful EHR user” under 42 CFR 495.4, which require eligible professionals to report on Clinical Quality Measures selected by the Centers for Medicare and Medicaid Services using only certified EHR technology, as part of being a meaningful EHR user under the Medicare EHR Incentive Program. EHR use by providers is already rather substantial. According to the Office of the National Coordinator for Health Information Technology, in 2015, 96 percent of all non-federal acute care hospitals possessed certified health IT. While small rural and small urban hospitals had the lowest rates at 94 percent, 96 percent of critical access hospitals had certified health IT. Clearly, EHR vendors and their products are an integral part of data usage and PHI confidentiality, the keystones of data governance efforts. Data governance: key component of care delivery models Many healthcare organizations struggle with data governance. A 2014 American Health Information Management Association (AHIMA) survey of over 1,000 healthcare professionals revealed only 11% characterize their data governance programs as being mature while over 50% of the respondents did not have governance practices in place.[i] The Health Information Management and Systems Society (HIMSS) has an excellent resource on overcoming data governance obstacles. The article is entitled, “A Roadmap to Effective Data Governance: How to Navigate Five Common Obstacles” and defines data governance as “the exercise of decision-making and authority for data-related matters.” [ii] The article analogizes the importance of having an effective data governance program seamlessly embedded within the overall management and operational practices to patient safety as an integrated component of a comprehensive care delivery model in any healthcare system. One obstacle identified is not addressing data governance from an enterprise perspective, which can perpetuate data integrity challenges. Data integrity: accuracy, quality, and completeness Assuring data integrity is certainly an essential component of data governance. Data integrity is defined by the Department of Health and Human Services’ Office of Civil Rights as “the property that data or information have not been altered or destroyed in an unauthorized manner.” Note that the alteration is not limited to intentional alteration; unintentional or mistaken alteration can compromise data integrity. Data integrity is particularly challenging for both providers and EHR vendors when it concerns patient identity. Accurate patient identity is an imperative. Health information exchange cannot be accomplished in a manner that assures integrity without first assuring patient identity integrity. AHIMA defines patient identity integrity as “the accuracy, quality, and completeness of demographic data attached to or associated with an individual patient. This includes the accuracy and quality of the data as it relates to the individual, as well as the correctness of the linking or matching of all existing records for that individual within and across information systems.” While data integrity must be the cornerstone of any institutional health provider’s data governance principles, individual healthcare providers must communicate often with their EHR vendors to be certain that the correct patient’s health information is the information being exchanged. Data dissemination: the call to collaborate with vendors The final area regarding data governance concerns data dissemination. This area has the greatest potential for achieving excellence for providers by nurturing a strong partnership with EHR vendors. Data dissemination is occurring at unprecedented rates, and its future upward trajectory is projected to be even greater. MACRA includes a provision that expands the availability of Medicare claims data which took effect on July 1, 2016. This section expands how qualified entities will be allowed to use and disclose Medicare data under the qualified entity program. Another MACRA provision that advances data dissemination is one that aligns with earlier efforts promoting interoperability. The tenets of the Certified EHR Technology criteria, which promote application programming interfaces that allow for interoperable data sharing necessary for big data analytics and population health management, will likely be coupled with MACRA’s Advancing Care Information (ACI). ACI will count for 25 percent of the Merit-Based Incentive Payment System (MIPS) attestation score in the first year of participation. MIPS advances population health management and care coordination by utilizing health IT that relies on open application programming interfaces (APIs) and an app-based approach to technology. Because APIs can be customized, providers will need to join forces with EHR vendors if they are to realize the financial benefits afforded by MIPS. Conclusion In summary, true data governance will not be possible without a strong partnership with EHR vendors. The partnership must go far beyond payment for services and assuring a business associate agreement (BAA) is executed. The BAA must be customized so that both parties have a meeting of the minds regarding data governance and other important factors that are memorialized in writing. Strong data governance must involve meaningful EHR vendor participation if it is to be sustainable. Community Care Network of Virginia, Inc. (CCNV), a community health center-owned and governed provider network, was legally incorporated as a statewide network organization in 1996 consistent with the Affiliation Policies of the Bureau of Primary Health Care. CCNV has a long, successful history of providing integrated, network-based services and programs to Virginia’s health centers, including the acquisition and implementation of a centralized practice management system, help desk, and support infrastructure commencing in 1999. Rene Cabral-Daniels currently serves on the NCHN board of directors. [1] Cohasset Associates, "2014 Information Governance in Healthcare Survey." American Health Information Management Association, May 2014; at http://www.ahima.org/~/media/AHIMA/Files/HIM-Trends/IG_Benchmarking.ashx
[2] See 'definitions of Data Governance.' The Data Governance Institute; at http://www.datagovernance.com/adg_data_governance_definition/
2 Comments
 Tis the season to be grateful. Here are just a few of the reasons we have to be grateful for this year.  I am grateful, appreciative and impressed with the Minnesota hospitals that are participating in the Integrative Behavioral Health (IBH) project! As a former clinician, I know the difficulty addressing behavioral health issues, especially when resources are limited. I also know the impact they have on the individual’s quality of life as well as the lives of their families and communities. Thank you for all you do! -Rhonda Barcus I would like to send a thank you to all the networks across our country who are working at improving the access to health care for rural America. The diversity of projects and locations makes it a fascinating group to work with. Their outcomes are amazing. We will have a healthier population in Rural America because of them. -Debra Laine I am grateful for our rural health partners that work with The Center to support the power of rural (FORHP, NRHA, NOSRH, RHIHub, Rural Health Value, Flex Monitoring Team, NCHN, NORC). I’m incredibly inspired by and grateful for The Heart of New Ulm Project, born out of New Ulm, MN. The 10-year initiative is producing financial and health outcomes that are preventing disease versus treating it after it occurs. The project was just awarded the Most Meaningful Life-impacting Improvement award at the Health Analytics Summit. This rural community is a perfect example of how collaboration and partnerships really can change an entire population’s health! -Kim Nordin  I’m grateful for all of the organizations and groups like the National Center for Farmworker Health, Research for Indigenous Community Health Center, Arizona Rural Women’s Health Network, and countless others that work to improve the health of vulnerable populations, including rural communities. It’s inspiring to see their outcomes and accomplishments. -Becky Gourde I’m grateful and amazed by the passion and persistence of those we work with here at The Center. No matter what our mission and vision statements say, we’re all shooting at the same target; enabling our rural providers to provide the very best quality of care to their communities and keeping rural areas healthy and vital. -Nicole Clement  Thank you to the thousands of rural health providers (hospitals, clinics, community health centers, health professionals, including EMS volunteers and community health workers) who are dedicated to providing care and improving health outcomes in rural America. -Sally Buck I’m grateful my grandparents have a critical access hospital in the next town from where they live, instead of the next closest hospital another 30 miles away. -Phil Birk  I’m grateful for the honor of working to support rural health care. It is an honor to work in an industry that makes a difference in the lives of 2.5 million people not only at just one point in time - they day they are seeking care - but for their future and the future of their loved ones.
-Tracy Morton I am grateful to the Minnesota Accountable Community for Health (ACH) Teams. These 15 teams have worked so diligently over the past three years to provide Minnesotans with better value in health care through integrated, accountable care using innovative payment and care delivery models. The work they’ve done is not only ground-breaking but truly inspiring. True leaders and pioneers in rural health. -Angie LaFlamme This article was written by Sally Buck, Chief Executive Officer at the National Rural Health Resource Center Today is National Rural Health Day, an event coordinated by the National Organization of State Offices of Rural Health (NOSORH) to Celebrate the Power of Rural. The National Rural Health Resource Center (The Center) is proud to support this important day by highlighting the community-based solutions and committed providers that overcome the unique health care challenges that rural citizens face. These challenges include a shortage of primary care and mental health physicians and dentists as well as higher rates of poverty and uninsured.
Rural providers are committed to the goals of the United States Health and Human Services, Centers for Medicare and Medicaid Services (CMS) initiative of Better Care, Smarter Spending and Healthier People.[1] At The Center we have seen this demonstrated by working with hundreds of rural health networks, small rural hospitals and State Offices of Rural Health (SORH) as a grantee technical assistance provider. Despite critical access hospitals (CAH), community health centers and rural health clinics being left out of many new innovation payment and care models initially due to their low volume or cost based reimbursement structure, there are many organizations leading the way towards value-based payment and care with an emphasis on quality and outcomes. These include:
Key partners for The Center are SORHs and state Flex Programs in our work to support rural communities and providers with services, information and resources to increase collaboration, improve quality reporting and improvement, recruit health professionals and support access to care by stabilizing hospital operations and finances through technical assistance, education and funding. This national network of rural health organizations and leaders are key to the power of rural. We see that our vision of “collaborating and innovating to improve the health of rural communities” is happening throughout the country through the dedication, innovation and partnerships and strongly demonstrates the power of rural. [1] CMS (2015). Better Care. Smarter Spending. Healthier People: Paying Providers for Value, Not Volume [fact sheet]. [2] Mueller, Keith and Fred Ullrich (2016). Spread of Accountable Care Organizations in Rural America, Brief No. 2016-5, RUPRI Center for Rural Health Policy Analysis. [3] Mueller, Keith and Fred Ullrich (2016). Spread of Accountable Care Organizations in Rural America, Brief No. 2016-5, RUPRI Center for Rural Health Policy Analysis. [4] Rural Health System Change Embedded in State Innovation Models (2016) Keith Mueller, RUPRI Center for Health Policy Analysis, Rural Health Value, [PDF - 494 KB] This article was written by Becky Gourde, program coordinator at the National Rural Health Resource Center/Rural Health Innovations, for the November 2016 edition of “Networking News.” The Network Technical Assistance Project is funded by the Federal Office of Rural Health Policy, Health Resources and Services Administration, U.S. Department of Health and Human Services through a contract to Rural Health Innovations, LLC, a subsidiary of the National Rural Health Resource Center. 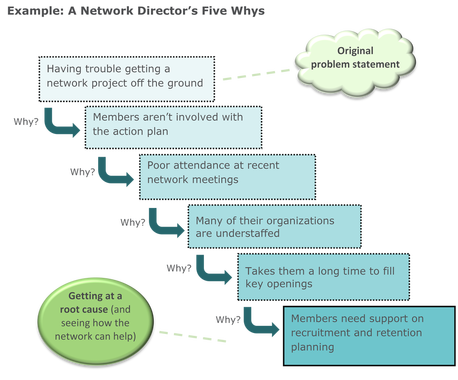 Rural health networks are often formed in response to collective challenges or needs arising out of the communities they serve. As part of health care’s current transition from a focus on volume to a focus on value, networks help drive and facilitate performance improvement efforts that contribute to CMS’s approach of Better Care, Smarter Spending, and Healthier People throughout the delivery of health care. Because Lean efforts usually require little, if any, direct financial investment, the related processes and tools can be a useful option for small organizations working to improve the health outcomes of their rural communities. What is Lean? In short, Lean is first and foremost a way of thinking that helps solve problems. Many of the ideas that we now categorize as “Lean” were developed out of the automaking industry. Shortly after World War II, Toyota began developing the Toyota Production System, or TPS, which was influenced by several thought leaders in industrial engineering. Although most people associate Lean with the practice of reducing waste and improving process efficiency, at the heart of the Toyota philosophy are a group of management principles characterized by (1) continuous improvement and (2) respect for people. Their success with the system inspired other automakers and eventually other industries to adopt similar techniques. (Lean is often associated with a similar methodology called Six Sigma, which was developed in the US in the 1980s and 1990s.) Specialized systems of Lean (Lean Healthcare, Lean Sigma Healthcare, etc.) focus on applications particular to the processes involved with caring for patients. Applying Lean to rural health networks For networks with a small number of staff (if any), modest infrastructure, and little influence on the direct provision of patient care, how can network leaders derive benefit from learning about the principles and practices of Lean? Interestingly enough, the Lean way of thinking dovetails with the objectives of rural health networks and provides new approaches for building network capacity. The actions listed below offer ideas for how networks can use Lean practices to their best advantage. 1. Tackle complex problems One of the notions of Lean is that problems are best solved when groups of people representing diverse roles or perspectives come together to identify issues and implement actions to address those issues. This format of problem solving is a common benefit arising out of rural health networks: networks often serve as ideal settings for candid and strategic discussions regarding the challenges being faced in the community. The network participants around the table have the power to collectively enact solutions that take into account multiple factors and perspectives. The key to addressing problems using Lean is to work on the underlying root causes under your control, rather than wasting time developing plans to alleviate 20 or 30 symptoms of those root causes. There are several Lean tools that facilitate the process of root cause analysis in ways that offer simple frameworks for dialogue and planning.
2. Lead a culture of continuous improvement Networks function most effectively when they help articulate members’ shared vision for the future of their communities. A shared vision expresses an ambitious and hopeful destination that all members are committed to using as a beacon for developing strategies and activities. The vision and goals are revisited periodically to assess progress and appropriateness, with new goals or elements revised as progress is made and circumstances change. This iterative process of striving toward better and better outcomes is at the very core of Lean principles. Network leaders are often in the position of facilitating and carrying forward that drive. Understanding Lean’s models for nurturing a mindset of continuous improvement can help guide network leaders through culture reinforcement and change management efforts among members. In fact, culture is often regarded by Lean experts as the highest priority for organizations wishing to become more effective and efficient: without an open commitment to progress and the empowerment of all participants to take part, performance improvement efforts are doomed to failure. According to Toyota, this transformation can be accomplished through the “respect for people” principle. Network leaders may recognize the tenets of “respect for people” as their own best practices for network collaboration:
3. Offer education As central sources for knowledge sharing, networks often allow member organizations to pool resources to pay for training or education that they otherwise couldn’t afford on their own. Because Lean has shown such positive outcomes throughout health care, coordinating and hosting educational opportunities on performance improvement can be a valuable service provided by a network to participating members and partners. The existing network configuration also provides a natural support system for members to get ongoing input from network leaders and from one another as they implement projects to improve outcomes in their own organizations. If performance improvement support is something a network is interested in pursuing as a value-added service, it may even be a worthy investment for a network director to become certified in Lean or Lean Six Sigma so that they can serve as trainers and project leads for members, preventing members from having to seek out external consultants on a case-by-case basis. 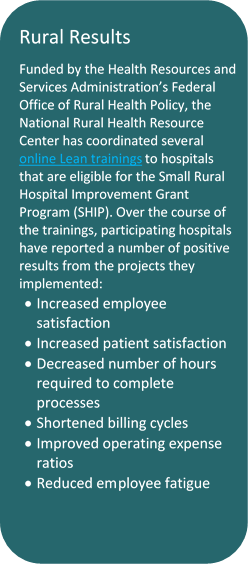 4. Gather and share outcomes Part of tracking the outputs and outcomes of a network’s work includes selecting measures and gathering data. The “simple” task of determining which metrics are most appropriate can be an intensive and tiresome process in and of itself, before the data collection even begins. Lean training incorporates an entire emphasis aimed at supporting users in what makes a good metric and which factors to consider. Many of the recommendations around Lean metrics offer valuable guidance for networks involved in evaluation planning:
It’s also helpful for a network to serve as a repository of member data on selected measures that are relevant to the network’s goals. This process of collecting and sharing member information can encourage benchmarking and sharing of best practices among member organizations working in similar areas. The information-collector role also allows networks to collect the designs of and results from the various improvement efforts being undertaken by member organizations, providing members with a quick way to see what’s been working well (or not so well) in their regions. Getting started You don’t have to become an expert to begin benefitting from an awareness of Lean principles and tools. In fact, performance improvement efforts are often most effective when you start small. If you’ve never been introduced to Lean or a similar methodology before, you may want to look into free or low-cost leaning opportunities (like books or online resources) to see if it would be a valuable investment in your professional development. Or if there’s someone within your network’s member organizations with a background in Lean, you could consider inviting them to a network meeting to review a few ideas that are relevant to a particular network initiative. Selecting one or two new performance management tools to practice with can also help you decide whether to seek out additional training or expertise. References
Jamie Martin, Lean Six Sigma Black Belt, SigmaMed Solutions John Roberts, Lean Healthcare Black Belt, Midwest Health Association Management Lean Hospitals: Improving Quality, Patient Safety, and Employee Satisfaction by Mark Graban, 2009, Productivity Press The Six Sigma Book for Healthcare: Improving Outcomes by Reducing Errors by Robert Barry, Amy C. Murcko, and Clifford E. Brubaker, 2002, Health Administration Press The Toyota Way: 14 Management Principles from the World’s Greatest Manufacturer by Jeffrey K. Liker, 2004, McGraw-Hill |
The National Rural Health Resource Center (The Center) is a nonprofit organization dedicated to sustaining and improving health care in rural communities. Rural Health Innovations, LLC is a subsidiary of the National Rural Health Resource Center. Archives
April 2017
Categories
All
|
 RSS Feed
RSS Feed
