|
The National Rural Health Resource Center (The Center) joins the National Organization of State Offices of Rural Health (NOSORH) in celebrating National Rural Health Day. National Rural Health Day showcases rural America by increasing awareness of rural health-related issues and promotes solutions that address them. Sally Buck, CEO of The Center, stated, "We have seen the power of rural through the innovative projects by health networks and small hospitals as they improve access and health outcomes through performance improvement in quality, finance, operations and health system delivery. There are many organizations across the country leading the way towards value-based payment and care with an emphasis on quality and outcomes." Through partnerships with SORHs, networks and state Rural Hospital Flexibility (Flex) Programs, The Center supports rural communities and their health care providers with services, information and resources to increase collaboration, improve quality reporting and improvement, recruit health professionals and support access to care by stabilizing hospital operations and finances through technical assistance, education and funding. "We see that our vision of collaborating and innovating to improve the health of rural communities is happening throughout the country," Sally said, "And strongly demonstrates the power of rural."  The Center has pulled together hospital and network spotlights from the past year to recognize the work that is being done and the positive impact it is having.
Technical Assistance and Services Center (TASC) Critical Access Hospital (CAH) Recognition
Additional information about National Rural Health Day can be found at www.powerofrural.org and to learn more about NOSORH, visit www.nosorh.org.
20 Comments
Optimizing Workflows to Share Data Across Sectors: Promising Approaches to Improve Care Coordination11/1/2017 Written by Jenna Frkovich, MPH, Data Across Sectors for Health (DASH), Illinois Public Health Institute  HealthInfoNet HealthInfoNet To provide coordinated care that meets patients’ needs, many networks and communities are developing information systems to share data across clinical and social service settings. In order for these systems to be effective in connecting patients to the right services at the right time, care teams need access to relevant individual-level data that is seamlessly incorporated into their work process.
Data Across Sectors for Health (DASH), a Robert Wood Johnson Foundation funded initiative, was launched to support multi-sector collaborations in sharing data to improve health. Of the ten collaborations that have received support from DASH, five are focusing on improving care coordination between medical and community services through enhanced information sharing that helps orient care around the whole person, not just their healthcare needs. As these collaborations moved from planning to implementation, they generated several lessons related to adapting new workflows based on integrated data and developing end user trainings. Getting Started When designing a new care coordination workflow, it is important to answer the following questions:
Depending on the environment, care teams may choose to: 1) design workflows around existing technology capabilities or 2) build new technology to fit new workflow needs. It will be important to determine early on the infrastructure and data required to modify workflows. Four of the five DASH collaborations chose to create new data collection forms for their workflows, while one chose to integrate existing data sources into their system. Some common technical tools that were used to coordinate care included shared plan of care documents, automated alerts and notifications sent across systems, and analytics that draw on multiple types of data to predict risk and identify people in need of more intensive services. Approaches that Work Below are five promising approaches taken by DASH collaborations—all of which have unique target populations, goals, partners, and resources, yet are collectively generating lessons with respect to multi-sector data sharing, specifically for care coordination. 1. Understand what end users value and gain their buy-in early on. Before HealthInfoNet set out to develop a new workflow for integrating social determinant data from Community Action Agencies (CAAs) into their state health information exchange, they documented how the CAAs were already collecting and using data for other purposes as part of their existing workflow. For example, they began by focusing on Head Start data that is already collected during the regular enrollment process and explained the clinical value of this data for at-risk pediatric populations. Taking time to understand the staff’s needs and how the new workflow could add value to their existing data rather being burdensome was key to gaining their buy-in. Read more » 2. Ensure community voices are heard during the process development. For Altair Accountable Care Organization (ACO), designing a new care coordination workflow began with understanding the personal preferences of the individuals served as well as those of their care team members. To inform the development of an e-Health infrastructure to coordinate mental and behavioral health services for people with intellectual and developmental disabilities, they gathered input from their clients about who should be on the multi-sector support team, what types of behavioral health events care team members should be alerted about, and how they should be guided to act on those events. Read more » 3. Choose a workflow that minimizes extra steps or makes work processes easier. The Center for Health Care Services, a mental health authority in Bexar County, TX, developed an alert system to notify behavioral health case managers when their clients arrive at emergency departments so that they can intervene earlier and prevent inappropriate hospitalization. By doing so, they automated the manual entry or list management that is often required of their case managers, saving them time to attend to clients. Read more » 4. Communicate roles/responsibilities clearly to all stakeholders. When the White Earth Nation began implementing WECARE, a care coordination database that screens families on the reservation to a wide range of community services, it was imperative that various tribal programs work in partnership when forming a comprehensive care team around the client’s priorities. Having great educators who could effectively discuss the benefits of WECARE, explain how to implement the screening, and work through any challenges with 800 staff from different community programs has been instrumental in building the momentum needed to implement WECARE reservation-wide. Read more » 5. Test and retest your process and allow for edits by people who complete the workflow. When the Parkland Center for Clinical Innovation, a part of Parkland Health and Hospital System, began recruiting participants into a program to share patient data between hospitals and food pantries, the health system originally led the recruitment effort. However, social workers found that providers were more focused on treating patients’ clinical needs and were not responsive to food security screenings. Instead, they decided to recruit participants from food pantries where individuals were more comfortable and accustomed to discussing social needs. Read more » Learn more DASH has learned from these grantees how to design new care coordination workflows when leveraging new data sharing technologies. You can find more in-depth descriptions of these projects in our new issue brief, Coordinated Whole-Person Care that Addresses Social Determinants of Health. Additional resources and updates about sharing data across sectors to improve health are available on our website. Jenna Frkovich, MPH, is the Communications Associate at the Illinois Public Health Institute, where she leads the development and execution of the communications strategy for Data Across Sectors for Health (DASH), a national initiative of the Robert Wood Johnson Foundation. DASH aims to align health care, public health, and other sectors to systematically compile, share, and use data to understand factors that influence health and develop more effective interventions and policies. Ms. Frkovich works to engage and grow a nationwide network of stakeholders by disseminating lessons learned, stories, and promising practices to help advance the field of multi-sector data sharing. By Robert Nelson, CAE, Founder and President of Nelson Strategic Consulting (NSC). This article was originally published on the NSC Blog.  Groupthink is a phenomenon that acts as a barrier to good governance. It is a form of self censorship that causes a failure of critical thinking when the desire for group consensus overrides one's ability or desire to critique / challenge a position, present alternatives or express an unpopular opinion. It is often in play when groups reach consensus without critically examining an issue; there is an illusion of agreement or consensus: “It appears as everyone agrees, so let’s move on.” It occurs when there is a high level of group cohesion or a strong persuasive leader who articulates his or her opinion, especially when the opinion is expressed early in the discussion. It also occurs when groups are isolated from contrary opinions. Board meetings are perfect breeding grounds for groupthink. After all, healthy boards experience a sense of team and cohesion, and they are often comprised of strong leaders. Paradoxically, this sense of cohesion can cause boards to fail in their fiduciary duty, if they consciously or subconsciously engage in groupthink. Creating a culture where disagreement and diverse opinions are valued limits the incidence of groupthink. Likewise, encouraging an atmosphere of open inquiry and fostering an open climate of dialogue are important protections. However, there are many more techniques that can be used to protect against groupthink. Protection Techniques:
Robert Nelson, a Certified Association Executive (CAE) and principal of Nelson Strategic Consulting, brings over a quarter-century of successful executive leadership experience, working with Boards and high-powered CEOs in a not-for-profit setting. He is adept at designing governance structures and an engaging Board development trainer. Nelson brings hands-on experience guiding and facilitating the development of solutions to complex organizational challenges and global grand challenges for national as well as international organizations. As a former association chief executive officer for almost two decades, Nelson understands the importance of developing practical, strategic solutions that work within the culture of an organization and are aligned with the organization’s capacity potential.
This article was written by Esther Hammerschlag, MA, owner of East Chewuch Consulting, for the September 2017 edition of “Networking News.” The Network Technical Assistance Project is funded by the Federal Office of Rural Health Policy, Health Resources and Services Administration, U.S. Department of Health and Human Services through a contract to Rural Health Innovations, LLC, a subsidiary of the National Rural Health Resource Center.  Network development is an iterative and dynamic process that doesn’t typically follow a straight trajectory, meaning an evaluation plan which only tracks numbers won’t paint a complete picture of your network. I like to think of evaluation first as telling the story—a story that is then backed by numbers. Although people may argue the benefit of one type of data over another (quantitative v. qualitative), the reality is you need both to tell the full story of your network. While numbers provide measurements across time, contextual and anecdotal information bring your numbers to life. Finding this balance and artfully merging the two is where you can most successfully demonstrate your network’s value. To accomplish this as a network evaluator, I like to administer surveys to members and/or stakeholders that include both closed-ended (e.g., multiple choice or scales) and open-ended questions. This allows me to:
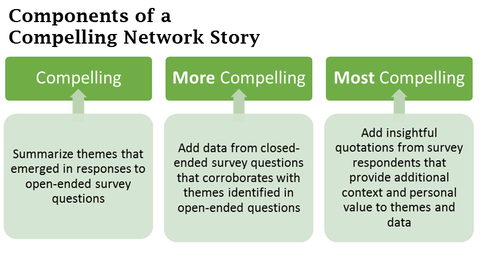
Collecting and analyzing qualitative data As an example, I recently completed a one-year follow-up evaluation of a relatively new, informal network that was working to improve its infrastructure and capacity. As one way to demonstrate value, I included an open-ended survey question asking members to describe how they had personally benefitted from participating in the network. I analyzed their responses using the same themes identified in last year’s survey, to allow comparison from one year to the next. By doing so, I found that an increasing number of members realized benefit from the network: almost half of members cited close ties to their own personal, professional, and organizational goals (nearly double than in 2016), and two-thirds indicated an increase in their own skills, knowledge, and awareness (an increase from 50% in 2016). I then looked at responses to a multiple-choice question asking members how much they agreed or disagreed with the statement, “The goals of the coalition support the goals of my own organization.” More than double the percentage strongly agreed with the statement in 2017 than did in 2016. (Do you see the pattern emerging?) Knowing organizations want to see numbers—and changes over time—I developed a graph showing progress in these indicators from 2016 to 2017. These indicators could continue to be measured in future years by asking the same questions, analyzing responses the same way each time. This graph shows how you can translate qualitative (descriptive) data into numerical displays of network value and progress over time. Several members also provided valuable comments in their responses, especially as to how participation has helped them within their own organizations. One member said, “Having the opportunity for professional growth has benefited the work I do both inside and outside the coalition,” and another stated, “It has kept me in the loop about how these challenging issues are affecting our community and our agency's population.” 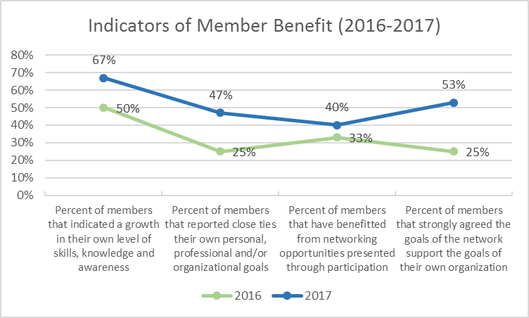 Turning data into a story You can begin to see how this network’s data emerges into a story. Using this example, the following passage about member benefit could be used in newsletters, annual reports, or relevant funding applications (names were changed for the purposes of this article): “Not only do an increasing number of our members feel the goals of the network support the goals of their own organization, but a growing number of our members indicate an increase in their own skills, knowledge and awareness. In fact, two-thirds of our members in 2017 cited an increase in their own skills, knowledge and awareness as a result of network participation, and more than double the number of members in 2017 as in 2016 strongly agreed that the goals of the network support the goals of their own organization. According to Joe Smith, CEO of Rural Community Hospital, ‘Having the opportunity for professional growth has benefited the work I do both inside and outside the coalition.’ Lucy Brown, the Executive Director of Family Planning Clinics states, ‘It has kept me in the loop about how these challenging issues are affecting our community and our agency's population.’” You could develop similar vignettes for other elements of network value using the same approach. For example:
 Identifying the right data to collect Before you develop a survey to collection evaluation data for your network, make sure to clearly define your goal. For example, do you want to quantify benefits to the community? Do you want to quantify challenges your network has faced, and demonstrate how you’ve overcome these challenges? Or do you want to evaluate strengths and challenges related to your network’s infrastructure and leadership? Some of my favorite open-ended questions to ask when evaluating networks are:
Responses to these types of questions can be sorted into themes and then quantified, as in the example I showed you. To provide additional measures that corroborate these themes, some of my favorite closed-ended questions use scales. For example:
Finally, think about developing dashboard tools as you write your surveys. How might responses to questions be turned into data points that can be tracked over time? Whether you want a big-picture snapshot of your network’s value, or you want to hone in on something more specific, using this approach will help you tell your story in a compelling way. Sharing a compelling network story is one of the best ways to maintain engagement and participation of your members and stakeholders, strengthen funding applications, and gain financial backing from your members by personalizing your request to make it more meaningful. Esther Hammerschlag, MA, is the owner of East Chewuch Consulting and provides a variety of program planning and development services for health and social service programs, including strategic planning, community health assessment, and program evaluation. As a former network director, she has a special interest in working with health networks that are working to improve the health of rural communities. She brings over 17 years’ experience in the planning and implementation of a variety of health and social service programs from the perspectives of consultant as well as community facilitator, and holds a master’s degree in Rural Development from the University of Alaska Fairbanks with a focus on creating effective and meaningful collaboration to improve community health
Written by Angie LaFlamme, Senior Program Coordinator, National Rural Health Resource Center/Rural Health Innovations  Rural Health Innovations (RHI) worked with ASPIN and their member health care organizations on collaboration in their behavioral health technician recruitment and retention efforts during an on-site visit on June 15, 2017. Clockwise from top left: Paul Conrad, Director of Training and Workforce Development, ASPIN; Robb Backmeyer, COO of Recovery Services, Centerstone; Ben Hall, Senior Talent Acquisition Business Partner, Centerstone; Chris Morrison, ARRC Project Coordinator, ASPIN; Eric McCray, Recruitment Coordinator, Bowen Center; Angie LaFlamme, Senior Program Coordinator, Rural Health Innovations; Kathy Cook, CEO, ASPIN; Amy Coplen, Employment Coordinator, Four County Counseling Center. Affiliated Service Providers of Indiana (ASPIN) is a 501(c)(3) nonprofit behavioral health provider and education network offering access to clinical providers in over 50 locations throughout the state of Indiana. As a result of being awarded a Health Resources and Services Administration (HRSA) Rural Network Allied Health Training grant, the network formed the ASPIN Recruitment and Retention Consortium (ARRC) in September 2015. ARRC brings key partners together to improve behavioral health and well-being among Indiana’s rural communities that experience health professional shortages. This June, Debra Laine and I traveled to Indianapolis for an on-site technical assistance (TA) visit with ARCC staff and partners, where we asked them to share information on their network’s best practices, lessons learned, challenges, significant outcomes and achievements, sustainability, and evaluation. Below are the accomplished and motivating responses we received from Kathy Cook, CEO/President, Paul Conrad, Director of Training and Workforce Development, and Chris Morrison, ARRC Program Coordinator. Q: What are some of the accomplishments you’ve seen during this grant project?
A: There has been notable impact having stemmed from the Employee Satisfaction Surveys feedback activities and the Health Care Organization’s Recruitment and Retention plan strategies that have been implemented. We have also had great success in our social media campaigns as well as alternative student recruitment strategies we’ve used for behavioral health student and employee recruitment. Our target marketing has been quite effective. Our executive leadership expressed buy-in from the beginning and has been very enthusiastic about the work we’ve done in bringing key partners together to improve behavioral health and well-being among Indiana’s rural HPSA [Health Professional Shortage Area] communities. Q: What challenges or barriers has your program encountered? A: Student recruitment has been a challenge of ours. The level of follow-through from the applicants can minimal at times. Navigating the many advertising/marketing mediums took some time. There was a lot of trial and error in ultimately determining which venues worked best for us in reaching our target markets. Our rural geography has also been a challenge. We target schools in rural areas to promote the awareness of Behavioral Health Technicians. Our hope is to recruit students into the educational training programs for this profession and upon graduation, placing them into the rural area clinics and hospitals. Q: How have ASPIN’s collaborations helped your program succeed? A:
Q: What lessons have you learned throughout the project? A:
Q: What have been some of ASPIN’s most significant outcomes? A:
Q: How is ASPIN approaching sustainability? A:
Q: On a scale of 1 (low) to 5 (high), how do you rate your network for sustainability following the grant program? A: We rate our sustainability at a five, by expanding the ARRC Network for continued collaborative work. Q: How are you implementing your evaluation plan? A:
Q: What are your major activities or initiatives for this year? A:
Q: What are a few of ASPIN’s best practices that you would like to share with other networks? A:
This article was written by Lydia Hooper of Fountain Visual Communications for the August 2017 edition of “Networking News.” The Network Technical Assistance Project is funded by the Federal Office of Rural Health Policy, Health Resources and Services Administration, U.S. Department of Health and Human Services through a contract to Rural Health Innovations, LLC, a subsidiary of the National Rural Health Resource Center. Networks are able to solve problems that individuals and organizations cannot on their own. Often when we think of them, we think about coordinated resources and activities, but we also need to think about the coordinated flow of information and ideas. After all, the reason networks are more effective at addressing large-scale issues is that multiple clusters of expertise can inform one another in order to be both more efficient and more responsive to needs. Just as human organs are composed of cells and tissues, networks are made up of individuals and organizations working together to perform various functions simultaneously. To do so, they need to be in consistent communication with one another. Communication in networks is different than in organizations. When we understand this, we can recognize and capitalize upon the incredible opportunities they present. Here are four ways communication is different for networks and four strategies for success. 1. Communication is multi-directional. In contrast to networks, the hierarchical organizations and systems we are accustomed to seek to maximize control and stability by having leaders decide what and how to share information, both inside and outside the organization. Unfortunately, these systems are breeding grounds for miscommunication and poor strategy because those who aren’t leaders also have valuable information that may not be fully utilized. Networks have an incredible opportunity to re-think how information and resources are used. Instead of looking to an executive, we can look to one another and assess what our goals are and how we might each contribute to get there. Organizations that participate in networks may find that it takes considerable effort to break habits based on organizational norms such as looking for clear directions to follow. Networks that use a collective impact framework may have a backbone organization leading coordination, but this can carry with it a risk that the other organizations will easily revert to the habits of traditional hierarchies that they are accustomed to. The solution: Develop an internal communications strategy. Sometimes networks put the cart before the horse by thinking about marketing or branding before they’ve focused on group clarity and coordination. Establishing group identity and an internal narrative will help your network progress, and it will also help those outside the network better understand what you are doing and why. A strategy should include your network’s shared goals and their coordinated plan for reaching it. A discussion about how resources will be shared should also include how external communication will be supported and executed, preparing the cart for when the horse is really to run. It is important to remember that communication both reflects and drives culture. One network I’ve worked with developed their strategic plan together, but then months later when the network was getting disorganized and losing focus, the plan was sitting on the shelf. A different one continues to reference their shared vision, even sharing best practices with other networks. 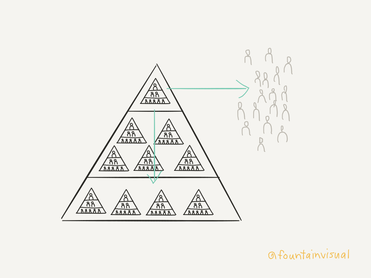 2. More people need to reach consensus internally. The strength and potency of networks is not measured by the number of people or organizations involved, but rather by whether there is sufficient diversity of thought and experience to create new solutions and maximize their potential for success. Having many different voices at the table can invite unique challenges such as:
Knowledge-based networks are all about leveraging what “who you know” knows, but before we can do that, we must first know what each of us knows. Sharing with other network members isn’t always easy, especially because our individual need to belong often eclipses our group need to accomplish tasks. But once many voices can learn to harmonize in unison, their volume will be difficult for anyone to ignore. The solution: Invest in building trust. Building trust takes considerable time. Networks may have to ask themselves, “Is it more important to accomplish specific tasks within a given timeframe, or is it more important to reach our goal?” Doing the latter may require sacrificing the former. Building trust also requires leaning into discomfort and conflict, which generally we try to avoid. I have found that the simplest, most effortless way to do this is to use a visual communication tool known as graphic recording to support group members in real-time with understanding complexity and feeling included. Graphic recording is real-time illustration that organizes information during group meetings, supporting members so they can share, understand, and retain more information. For example, one graphic recording I’ve created visually captured a meeting that was a turning point for two networks that had felt in competition with one another. While individuals arrived at the meeting skeptical about engaging in a facilitated process together, they used the visual to work through their conflicts and by the following year recognized the graphically recorded meeting as the one during which they came together as one. 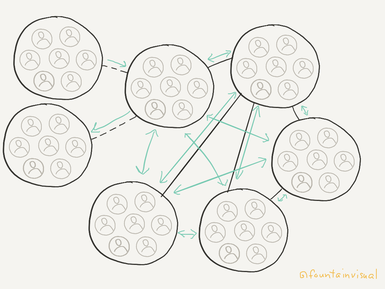 3. External communication is essential. Networks present opportunities to break through former communication barriers that impede progress, but they are still at risk of becoming isolated from the input of information they need to be effective simply because our natural inclination is to associate with those we are most like. Complex networks in nature demonstrate that long-term sustainability depends upon balancing efficiency and resilience. The hitch is that while efficiency depends upon the minimization of diversity and interconnectivity, resilience depends on the maximization of them. Likewise, communication in social networks must balance strengthening existing relationships in order to use current network knowledge and consistently creating new relationships in order to expand that knowledge. Whether your network thinks of this as partnership building, community stakeholder engagement, or marketing, keep in mind that communication is never one-way. Networks may provide information, but they can also get the information they need, for example about the effects their activities are having or the effects they could or should. The solution: Create new ties thoughtfully. Your network will need to apply the same patient, realistic, strategic approach that you practice internally to build relationships with external stakeholders. It is worth the careful consideration this takes in order to ensure that the work of your network stays relevant. Respect the time and contributions of others by thinking about what matters to them. If you seek to build bridges by empowering individuals to voice their concerns, then plan to address those concerns (or better yet to give them the agency to do so themselves) so those bridges don’t then get burnt. One network I’ve worked with is really great at using deliberate facilitative processes but is less practiced at producing early wins that keep stakeholders engaged and hopeful. Others I know can get so focused on producing certain outcomes by deadlines set by a funder, such as having a certain number of people attend meetings, that progress toward their primary goal, such as to have those people inform solutions that will work, is stunted. 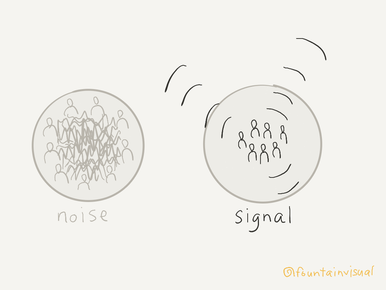 4. Messaging (including data) is dynamic. While the organizations that comprise them may focus on offers of services or products that solve concrete needs, networks are in the business of sharing ideas that are often complex and sometimes invisible. Furthermore, networks themselves are fluid, and as more information becomes available messages will need to change. Networks also have to communicate with multiple audiences, which can challenge individual organizations who may relate differently to them (for example, one organization in the network may rely upon a critical partner who is a perceived threat to another organization). The solution: Create structures for consistent learning and reporting. As their work ebbs and flows, networks need to stay focused on what’s currently happening. Through thoughtful collection and reporting of high-quality data (both quantitative and qualitative), networks can position themselves to be able to intentionally adapt.
I admire the networks I work with who are willing to dedicate adequate thought and resources to this development. I am saddened by those who get distracted by technical tools when they can start now, even with simple paper surveys, ensuring there will be some data to show change over time. The ones that I know are guaranteed to make a difference are those who are willing to discover what isn’t working and be open to change. That kind of resiliency is the very reason networks are capable of exceptional results. Lydia Hooper is a consultant who specializes in helping organizations collaborate and communicate about complex topics. She has partnered with more than 40 organizations and networks, offering services and trainings in data storytelling, graphic recording, and communications strategy. You can read more blog articles and get a free copy of her ebook “Using Visuals to Support Collaboration” at www.fountainvisualcommunications.com.
This article was written by Rene S. Cabral-Daniels, JD, MPH, CEO of Community Care Network of Virginia, Inc., for the July 2017 edition of “Networking News.” Isaiah Dolcee and Eliza Singleton, interns at Community Care Network of Virginia, also contributed to the article. The Network Technical Assistance Project is funded by the Federal Office of Rural Health Policy, Health Resources and Services Administration, U.S. Department of Health and Human Services through a contract to Rural Health Innovations, LLC, a subsidiary of the National Rural Health Resource Center The impact of health information technology (IT) on the healthcare industry is irrefutable. According to the Department of Health and Human Services’ Office of the National Coordinator (ONC), nearly 90% of office-based physicians have adopted an Electronic Health Record (EHR).[1] Moreover, the percentage of hospitals that provide patients the ability to view, download, and transmit their health records online accelerated from 10% in 2013 to 69% in 2015. Patients are likewise availing themselves of this resource in greater numbers. The ONC reports patient use of information technology to interact with their health care provider, view their personal health information, and track their health and wellness grew significantly between 2013 and 2014. Patient use of one or more of the selected types of IT significantly grew between 2013 and 2014, from 39% to 48%. The growth in EHR utilization by patients and providers alike likely reflects the many benefits of this technology. Providers value the ability to make medical decisions based on the most current information. As patients may receive care in a variety of healthcare settings, the ability to coordinate the most recent medical information in deciding future treatment is an imperative for providers. EHRs also enhance patient safety, particularly by assuring greater reliability in prescribing pharmaceuticals. Patients requesting their medical records through an EHR can expect to receive complete documentation free from handwritten notes that often prove difficult to read. The significance of interoperability within health care performance All of these benefits, as well as the benefit of cost reduction, help communities realize health system performance Triple Aim goals:
Interoperability of EHRs has the ability to enhance each of the Triple Aim benefits. The American Hospital Association asserts interoperability progress will support all three Triple Aim goals,[4] each of which has a positive impact on rural communities.  Enhancing the rural patient experience The challenge each Triple Aim criterion seeks to address is greater in rural communities; interoperability of electronic health records therefore has a greater advantage in rural communities. The first Triple Aim criterion, patient experience of care, may have a geographic correlation. A study of health center patients found urban patients were more satisfied with their physicians than rural patients.[5] This finding is likely influenced by the challenges faced by rural health providers. Rural American communities face substantial healthcare disadvantages compared to urban and suburban communities. The 40 to 45 percent of people who reside in these areas (approximately 150 million people)[6] report higher levels of chronic conditions and a lower per capita income. These factors, combined with the lack of specialists in rural communities, force many patients to travel to more populated areas to find certain providers. Patient care is often solely provided in the few hospitals in these areas, causing most to be overextended and under supplied. EHR interoperability can play an important role in enhancing patient satisfaction. The Rural Health IT Corporation asserts improving customer satisfaction in healthcare depends on complete data interoperability.[7] The Bipartisan Policy Center report on the role of health IT in transforming healthcare stated studies indicate high levels of patient satisfaction with online consumer tools.[8] Clearly, patient satisfaction can be positively influenced by EHR interoperability. This finding is particularly relevant to rural communities, as rural patients tend to be less satisfied with their care than their urban counterparts.  Improving the health of rural populations Improving the health of populations is the second goal of the Triple Aim. Population health management includes the methodologies for providers and payers to contain and lower costs, thereby increasing operational efficiencies such as the ability of providers to streamline care and improve treatment outcomes. One of the main benefits of EHRs is increased access to information.[9] Interoperability of EHRs escalates that benefit by assuring the information is comprehensive and not site-specific, a necessary element in improving population health. This advantage of comprehensive data review by providers is imperative for rural communities, as residents need to travel greater distances to access different points of the health care delivery system. Healthcare facilities in these areas are small and often provide limited services, thereby requiring rural residents to travel to seek care, particularly tertiary care. Often, due to geographic distance, extreme weather conditions, environmental and climatic barriers, lack of public transportation, and challenging roads, rural residents may be limited/ prohibited from accessing healthcare services in their communities.[10] Utilizing health IT has benefits for rural providers and patients alike. For example, patients can exchange secure messages, have “e-visits” with their physicians and decrease the hassle of traveling to a specialist. Specialty referrals are also made easier, which is valuable since access to them is often limited.  Reducing costs by increasing interoperability The third criterion of the Triple Aim involves reducing the per capita cost of healthcare. Every year, providers lose millions of dollars due to the amount of time spent searching for paper medical records. In the past, knowledge of a patient’s medical history relied on physical records held by a primary physician and the memory of a patient, both of which were not completely reliable. These inherent discrepancies in health data are even more prevalent in patients from rural areas since most tend to see multiple physicians. By increasing interoperability, time is used more effectively to solve a patient’s concerns and therefore save money for both the practice and the patient.[11] The Office of the National Coordinator’s Connecting Health and Care for the Nation: A Shared Nation Interoperability Roadmap stated interoperability can help reduce care delivery redundancy and cost by allowing test results to be reused while supporting analyses to pinpoint waste. The per capita cost of healthcare is significantly reduced with the implementation of interoperable EHRs. This is because patients no longer have to pay for both the cost of administering care as well as complex IT systems that are necessary to access health data in siloed information systems to administer effective care. The West Health Institute calculated the aggregate financial benefit to be projected at $30B saved in the healthcare industry per year.[12] Efforts to lower costs will therefore positively benefit rural communities as their local providers will have access to a full panoply of tests if interoperability of EHRs is complete. The nation as a whole benefits from true interoperability of electronic health records. When these benefits are viewed through the lens of the Triple Aim, the benefit to rural communities is even greater. Community Care Network of Virginia, Inc. (CCNV), a community health center-owned and governed provider network, was legally incorporated as a statewide network organization in. CCNV has a long, successful history of providing integrated, network-based services and programs to Virginia’s health centers, including the acquisition and implementation of a centralized practice management system, help desk, and support infrastructure commencing in 1999. With over two decades of experience as a leader in health policy, finance, and law, Rene Cabral-Daniels has been the CEO of CCNV since 2013. She currently serves on the Healthcare Information and Management Systems Society (HIMSS) North America Board of Directors as well as the National Cooperative of Health Networks (NCHN) Board of Directors. Isaiah Dolcee is a rising senior at Princeton University, and Eliza Singleton is a rising junior at Elon University. [1] Quick Stats by healthit.gov
[2] The IHI Triple Aim by Institute for Healthcare Improvement [3] National Alliance for Health Information Technology. “What Is Interoperability?” 2005. Available online at www.nahit.org [4] Achieving Interoperability that Supports Care transformation: A Report of the American Association Interoperability Advisory Group [5] Influences on patient satisfaction in healthcare centers: a semi-qualitative study over 5 years by Ruth D. Thornton, Nichole Nurse, Laura Snavely, Stacey Hackett-Zahler, Kenice Frank and Robert A. DiTomasso [6] Why Health IT Integration Must Assist Rural Healthcare by HIT Infrastructure [7]81% dissatisfied with healthcare, Interoperability can help by ruralhealthit.com [8] Transforming Health Care: The Role of Health IT (fix citation) pg 23 [9] Jamoom E, Beatty P, Bercovitz A, Woodwell D, Palso K, Rechtsteiner E. “Physician Adoption of Electronic Health Record Systems: United States, 2011.” 2012. [10] Healthcare disparities & barriers to healthcare by Stanford eCampus Rural Health [11]Healthcare Interoperability can reduce costs and improve care by iShare Medical [12]West Health Institute finds medical device interoperability could save more than $30 billion a year by West Health Institute This article was written by A. Craig Dixon, MS, and Ashley Vincent Poore, MA, of the Coalfield Regional Healthcare Network, for the June 2017 edition of “Networking News.” The Network Technical Assistance Project is funded by the Federal Office of Rural Health Policy, Health Resources and Services Administration, U.S. Department of Health and Human Services through a contract to Rural Health Innovations, LLC, a subsidiary of the National Rural Health Resource Center.  Okay, “big-idea people.” We know. You have a plan that is just what this company needs. It’s radically different, and it could change the way we do business – the way the whole industry does business. But why won’t anybody listen? “Big-idea people” trying to get buy-in for their plans can feel like Sisyphus, condemned to an eternity of rolling a boulder uphill, only to see it roll back to the bottom of the hill at the first sign of resistance. Let us offer some suggestions to overcome organizational inertia to get your project moving. Suggestion 1: Use data to define the problem. Chances are, the folks you are pitching your idea to are not going to be excited about your idea simply for its intrinsic value. You have to convince them it is going to solve a problem they care about. In fact, you may have to first demonstrate to them that there is a problem. How do you know there is a problem? What data brought you to your conclusion? While quantitative data (i.e., hard numbers) often represent the best way of communicating the problem, don’t underestimate the value of a couple of compelling anecdotes (qualitative data). Sometimes, a particularly bad experience or an incisive quote can be just as effective as a table of figures or a chart. Your data should answer the questions your audience is likely to have, and do so in a compelling manner. How bad is the problem? Is the problem worse locally than in similar locales elsewhere? How will we know if we have fixed the problem or mitigated its severity? What negative consequences will result if the problem is not addressed, and how bad could they be? What positive outcomes are possible if it is, and how could that benefit your organization? The aim of your data is to provoke emotion in your audience – emotions like empathy (“I have experienced a problem similar to this before”), outrage (“How can this problem exist/be this bad?”), or moral obligation (“It would be wrong to allow this problem to continue”). Once your audience is convinced that there is a problem that absolutely must be solved, they’ll be looking for ideas, and it just so happens that you have one.  Suggestion 2: Leverage your professional relationships. It is usually a good idea to build a core group of supporters around your idea before presenting it widely. When considering recruits for your team, think about who else would benefit from this idea being implemented. Who is also passionate about the issue being addressed? Getting passionate team members on board will broaden your potential impact and improve your credibility, helping your proposal’s chances of being successful. Think about the people you already know. You don’t have to go right to the top of your own or another company’s organizational chart. Reach out to people with whom you already have a good working relationship. You have a better chance to get buy-in from someone you already have a good rapport with. When you pitch the idea to prospective partners, don’t present them with a fully formed plan. Allowing your colleagues to help in the development gives them more investment in the proposal and increases their engagement. Even if input from others strays a bit from what you originally envisioned, a really good plan formulated by five people will almost always get buy-in faster than a perfect one created by one person. The opportunity to include their own agendas will possibly broaden the project into something more beneficial that you hadn’t previously considered.  Suggestion 3: Promote outcomes, not actions. No matter how elegant or brilliant your idea, far fewer people are likely to be interested in the idea itself as the outcomes it can produce. You should be prepared to talk about the latter at least as much as the former. Be realistic with what you believe you can accomplish. There is seldom one solution that completely solves a problem. You are just trying to take a bite out of the problem. How big will that bite be, realistically? Don’t sandbag so badly that no one gets excited about the idea’s potential, but it is often wise to under-promise and over-deliver. Doing the reverse can really damage your credibility. This is another place where a mix of quantitative and qualitative information can really help. First, try to quantify the benefits of implementing your idea (e.g., “We could save $10,000 per year” or “We could reduce downtime by 10 percent”). Then try to describe what your department, organization, network, or community would look like if these results were achieved. Who will be affected – within your organization and beyond – and how? What changes will they notice in their day-to-day lives? Seeing this complete picture can really help get people excited about your idea’s potential. Whether you’re proposing a grant project or working to get a group of partners together to solve a problem locally, we believe you will find these suggestions helpful in considering how to approach the process. By using meaningful data, including colleagues who will also benefit, and promoting the proposal’s potential outcomes, you can get your big-idea boulder “over the hump,” moving quickly and effectively from idea to implementation. Then, you can kick back and enjoy some well-deserved nectar and ambrosia. A. Craig Dixon is a grants specialist at Madisonville Community College (MCC) in Madisonville, Kentucky. Since transitioning to his current position in 2011, he has secured over $4 million in grant funding for the college from agencies such as the National Science Foundation, the Health Resources and Services Administration, the U.S. Department of Agriculture, and the Delta Regional Authority. He has been selected to present at national conferences hosted by the National Institute for Staff and Organizational Development (NISOD) and the League for Innovation in the Community College, and his work has been published electronically by the Council on Resource Development and the Kentucky Office of Rural Health. He holds a Master of Science in Computer Science from Western Kentucky University in Bowling Green, Kentucky, and a Bachelor of Science degree in Computer Science from Murray State University in Murray, Kentucky.
Ashley Vincent Poore is the Director of Education and Research at Baptist Health Madisonville (BHM) in Madisonville, Kentucky. Her 15-year career in education includes ten years at Madisonville Community College, first as an adult education instructor and later as director of the college’s assessment center. For two and a half years, she coordinated educational programs for the West Area Health Education Center in Madisonville, and in her present position with BHM, she oversees six departments, including a regional medical school campus, a family medicine residency program, a doctoral nurse anesthetist program, and an area health education center. She also serves as Network Director for the Coalfield Regional Healthcare Network – a group of leaders from medical and educational organizations that include a regional medical center, a critical access hospital, two federally qualified health centers, an area health education center, a mental health provider, and the local health department and community college. This article was written by Jo Anne Preston, MS, Workforce and Organizational Development Senior Manager at the Rural Wisconsin Health Cooperative (RWHC), for the May 2017 edition of “Networking News.” The Network Technical Assistance Project is funded by the Federal Office of Rural Health Policy, Health Resources and Services Administration, U.S. Department of Health and Human Services through a contract to Rural Health Innovations, LLC, a subsidiary of the National Rural Health Resource Center. The notion of the solitary, forceful leader who makes things happen is outdated for the way we want to do business today. Position power can make us comply – for a while anyway. But when what you really want is people joining your cause and kicking in (think: leading a rural health network), your real power lies in your ability to influence.  Understanding Motivational Styles through Personality Theory What we can do is “fuel” the motivational needs that others have, and one way to get better at this is through a basic understanding of personality theory. How one is wired in personality reveals unique information about the kind of fuel needed to get him or her motivated, and the conduit is how we communicate. Examine your communication style to see if you meet the needs of those whose motivation requires the following elements:
 Increasing your own influence There are many recipes for gaining influence, but they all have one vital ingredient: the ability to build relationships of trust. This article identifies a few opportunities to reflect on your own trust-building behaviors. Your credibility earned through trust is your secret sauce, and you can’t really influence without it. But trust doesn’t stand alone. How you handle yourself makes more difference than you might think, and it definitely impacts your ability to influence. We sometimes undermine our own credibility without realizing it. The following small steps can help us self-manage our actions to maintain credibility with stakeholders: 1. Ask for help. When you don’t ask others for help, they don’t get a chance for successful contribution, and then we may wonder why they are not engaged. This can also lead to feeling like you have to do everything yourself. “I could really use your help; would you be willing?” is a great way to influence and gain engagement. 2. Create space for others to lead. Ego can get in the way of effective power when we fail to create space for others to lead too. We need not be threatened by others’ power. Instead, find ways to access others with influential power to help you bring people on board. Take advantage of their relationships to make connections for you. 3. Manage stress. It can truly be said that we are not overwhelmed by life, but that we overwhelm ourselves with our thoughts about life. People sense our overwhelmed demeanor and run the other way. Break your initiatives down into clear milestones you can articulate so that you can “sell” something people can envision (and at the same time, enjoy less stress). 4. Appeal to their needs. Having a great idea is not enough to get people to sign up. There are competing needs for time and energy, and you can’t “should” someone into joining. If you find your frustration is getting the best of you, you may be trying to push a noodle uphill. What would appeal to them? How does it serve a need they have? Find a connecting story rather than a “should.” 5. Never use gossip as influence. If someone upsets you, listen to them instead of talking about it to others. They may have something you need to hear and may be in a position at some point in the future to help you. Gossip comes back like a boomerang. Gossip is influence, but not the kind that helps.  6. Be specific. Get better at specifically estimating the time or financial resource ask you are making, e.g., “This will take about 10 hours over the next 6 weeks.” It helps people discern and decide. 7. Start small. Getting a “yes” doesn’t have to be all or nothing. Take advantage of pilots where you try something out as a study to learn from it. Provide different tiers of what you offer to allow people to see some benefits without having to fully commit before they are ready. By becoming aware of the motivators of different personality types, building trust in our relationships, and taking manageable steps to maintain credibility, leaders can more effectively influence collaborators to support the work of the network.
Remember you already are having an influence. Is the kind of influence you want to have? List your assets. What do you have to offer as uniquely you? Make use of it, without over-relying on it. Any strength over-used can become a liability. Jo Anne Preston is the Workforce and Organizational Development Senior Manager at the Rural Wisconsin Health Cooperative (RWHC) in Sauk City, WI. RWHC serves rural hospitals in Wisconsin with a variety of products and services to support and enhance rural healthcare. Jo Anne’s work includes designing and delivering leadership education, leadership coaching, team facilitation and consultation around employee engagement and customer service. She also serves on a variety of workforce-related work groups in Wisconsin to address solutions to rural workforce shortages. She has a M.S. in Educational Psychology/Community Counseling from Eastern Illinois University. Written by Angie LaFlamme and Bridget Hart, National Rural Health Resource Center. This content originally appeared on the 3RNet website. The 3RNet’s mission is to connect health care professionals searching for jobs in rural or underserved areas with health care facilities. They strive to find the right job for professionals in areas where they will live and work comfortably. Some health care professionals entering the workforce have come from large, urban areas and have never practiced in a rural community. But, for University of Minnesota medical students participating in the Rural Physician Associate Program (RPAP), this isn’t the case.
RPAP is a nine-month, community-based educational experience for third-year medical students. Not only does it allow them to train in rural communities, RPAP students and their families get to experience all aspects of rural community life by living in their host towns during the training period. “RPAP was one of the most valuable experiences of my training,” said Maren Anderson, who participated in RPAP in fall 2016. “I've always felt I would be best served by training in the environment I plan to work in and for me that is rural Minnesota. I knew I was in the right place when we walked down the hallway of physician offices and they pointed at nearly every door, identifying that physician as either a University of Minnesota graduate, RPAP alumnus, or both. I was the only medical student there which gave me the benefit of the undivided attention of not just one preceptor or attending, but every practitioner I came into contact with.” RPAP students experience hands-on learning as they care for patients of all ages. They learn clinical medicine, procedures, community health, and the business of medicine. Students experience the full spectrum of rural medical care as they follow patients and their families through a disease process or pregnancy. “In the course of a day I might start the morning with an early surgery or c-section, then start clinic, possibly see a patient or two in urgent care, get called to the ER to sew up a laceration, finish out clinic and write my notes, visit a patient or two on inpatient, and then wrap up the day with a delivery,” said Maren of her RPAP experience. “I truly felt like a member of the team and got to know my patients and my fellow health workers. I felt so incredibly valued and supported during my time there. I also felt like I became a part of the community in a way that I haven't found since moving out of my hometown,” said Maren. “My official preceptor would have me over to his house for dinner regularly and I helped his family shear sheep to get ready for the fair. I joined a church choir there and a number of choir members became my patients, eagerly announcing to me during practice, ‘I'm coming to visit you next week!’” From populations ranging from 350 to 30,000, over 110 Minnesota communities have participated in the program as teaching sites with a majority having at least one RPAP alum. Practices vary from small family medicine clinics to large multi-specialty outpatient centers, and hospitals ranging in size from 15 to 140 beds. Students see patients in clinics, hospitals, emergency rooms, nursing homes, hospice, at home, and in the community. Each student is the only student in a community and therefore has a greater opportunity to gain hands-on experience in a variety of procedures and specialties. “When the Minnesota legislature sought a solution to the need for more rural physicians – particularly Family Physicians – in the late 1960’s, they were wonderfully wise to fund the establishment of the University of Minnesota Medical School’s Duluth campus program and the Rural Physicians Associate Program,” said Jim Boulger, Ph.D., Distinguished University Teaching Professor from University of Minnesota Medical School. Since RPAP’s inception in 1971, over 1,300 students have participated in the program, resulting in two out of three former students practicing in Minnesota, two out of three practicing in rural locations, and four out of five practicing primary care. Statistics show that health care professionals with an educational background in rural areas are more likely to practice in these areas once they enter the workforce. “These programs have been extremely successful models for training our rural Minnesota medical workforce. Now having trained more family physicians – many of them RPAP graduates - than any other medical school in the United States, the University is a proud partner with greater Minnesota in providing care for all of us,” quoted Dr. Boulger. Former RPAP student Maren states, “RPAP solidified my faith in my decision to become a rural physician because, for the first time since starting medical school, I felt that I actually understood what it means to be a rural doctor and how that shapes your life—and now I can't imagine wanting to do anything else.” University of Minnesota, Duluth and Twin Cities Campus’ medical students with an interest in family medicine, primary care, or rural medicine specialties are strongly encouraged to apply to the Rural Physician Associate Program. Visit the RPAP website to learn more about the Rural Physician Associate Program, or if you have interest in supporting the Program. |
The National Rural Health Resource Center (The Center) is a nonprofit organization dedicated to sustaining and improving health care in rural communities. Rural Health Innovations, LLC is a subsidiary of the National Rural Health Resource Center. Archives
April 2017
Categories
All
|
 RSS Feed
RSS Feed
